
A thoracolumbar laminectomy and fusion is performed through an incision on your mid to lower back. This procedure involves fully or partially removing pieces of bone called spinous process and laminae that surround the spinal cord and/or nerves. This is done to enlarge the space for and to help relieve pressure on the spinal cord and/or nerves. After the laminectomy is performed, natural or synthetic bone material can be added to help fuse the vertebrae. If successful, spinal fusion will typically take place in the weeks and months following surgery. In instances where there is instability, implants such as metal screws and rods can be added to help provide stability to the spine.
1. Incision and Laminectomy
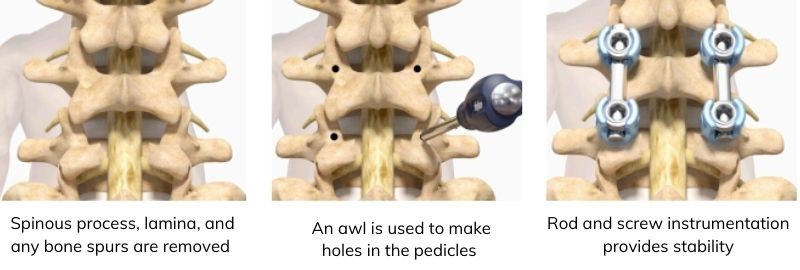
An incision is made along the midline of the back at the affected levels of the spine. After the spine is exposed, surgical instruments are used to remove the spinous process, lamina, and any bone spurs that may be intruding into the spinal canal. With these bones removed, the spinal nerves have more space, and the pressure on them can be reduced or removed.
2. Stabilization
Before supplemental bone material is added, instrumentation is introduced to help stabilize the spine. Either a drill or a sharp instrument called an awl is used to make holes in the bones connecting the back of the vertebrae to the vertebral bodies in the front of the spine. These bones are called pedicles, and the instrumentation placed into them are called pedicle screws. Pedicle screws are placed on both sides of the spine, and into the vertebrae above and below the laminectomy. Next, rods are positioned between the screws and fastened in place. The rod and screw instrumentation is designed to provide the necessary stability for spinal fusion to occur. If successful, spinal fusion will typically take place in the weeks and months following surgery.
3. Prepare for Fusion
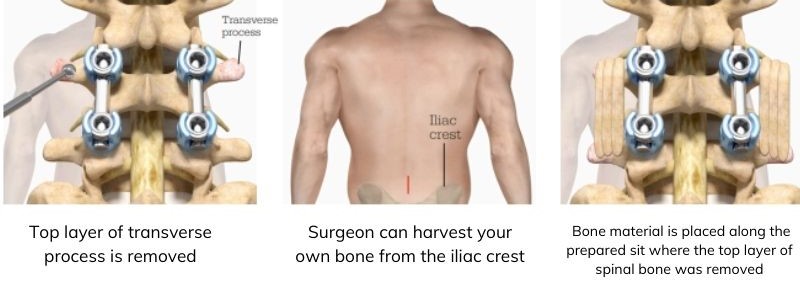
Once all screws are placed, a motorized instrument is used to remove the top layer of the transverse processes. This is the site where bone material for the spinal fusion will be added. Bone material can consist of pieces of a patient’s own bone (natural bone material), processed donor bone from a bone bank, or synthetic bone material. To harvest a patient’s own bone, either the original incision or a second incision made over the back of the pelvis allows the surgeon to remove bone from the part of the pelvis called the iliac crest and place it along the prepared site where the top layer of spinal bone was removed. Regardless of which type of bone material is used, the intention is for it to eventually grow in place, fusing the spine in the weeks and months following surgery and providing additional stability.
4. Surgical Closure
Your surgeon will close the incision and dress it with a wound covering at the conclusion of the surgery. Some patients require a brace, for a short period of time after surgery. As with any surgery, spinal surgery carries certain risks. Your surgeon will explain all the possible complications of the surgery, as well as side effects.